
Oregon’s prescription drug monitoring program doesn’t measure up to those in other states.
Risky prescribing practices have fueled Oregon’s opioid epidemic for years, while state laws have blocked some regulators from intervening.
An audit of the state’s prescription drug monitoring program released yesterday by the Secretary of State shows that state laws limit the Oregon Health Authority’s ability to investigate doctors and their prescribing practices. Modeled off initiatives in other states, Oregon’s monitoring program was established in 2009 to provide information about the use and abuse of prescription drugs. The audit found that the program lacks many of the tools available to regulators in nearby states.
The report also sheds light on the troubling extent of opioid addiction in the state and how it is enabled by some medical providers.
“I am personally heartbroken by some of the findings in this audit,” Secretary of State Dennis Richardson said in a press conference yesterday. “Oregon badly needs more tools to address the opioid crisis, reduce substance abuse, and help victims. We can do better, and this audit identifies concrete solutions that can help save lives.”
“I am personally heartbroken by some of the findings in this audit. Oregon badly needs more tools to address the opioid crisis, reduce substance abuse, and help victims.”
—Secretary of State Dennis Richardson
The drug monitoring program produces a database that could help prescribers identify a patient’s past drug use and limit harmful prescriptions. But state law does not require prescribers to use this tool. In the third quarter of 2018, only 39% of providers checked the database at least once.
“No one is required to access the [prescription drug monitoring program] database, voluntary usage is mediocre, and some key stakeholders can only access limited information and under very specific circumstances,” the authors of the audit wrote.
California, Colorado and Washington have made it mandatory to check their databases before prescribing opioids.
State laws block data sharing between the drug monitoring program and the licensing boards that oversee doctors and other prescribers. Even if researchers find out about abuse, they can’t tell the people who enforce the rules. Letters were sent to 160 problem doctors in 2018, but none of them were required to undertake additional education or training, or even reply to the letter.
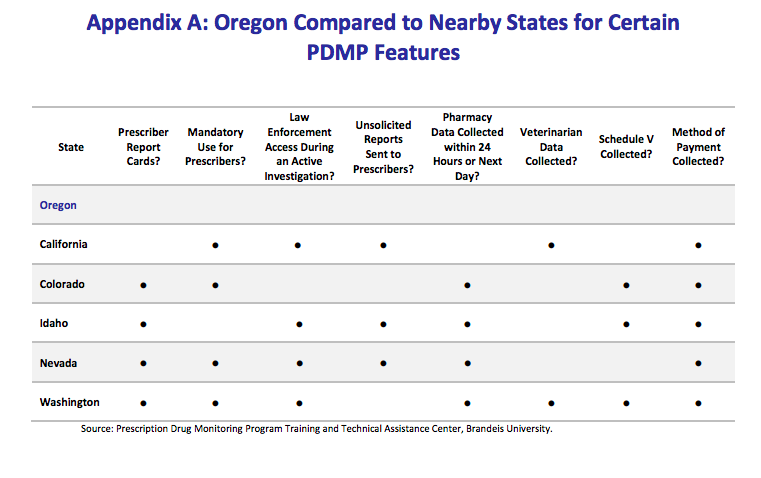 How Oregon’s drug monitoring program compares to other states. Secretary of State audit.
How Oregon’s drug monitoring program compares to other states. Secretary of State audit.
Law enforcement officers cannot access the data to help with their investigations. That makes it harder to identify and shut down “pill mills” and other lawbreaking.
The program only collects data from retail pharmacies like Fred Meyers, leaving a loophole for pharmacies at long-term care and residential treatment facilities. Some data were incomplete or difficult to access within a reasonable time.
As a result, risky prescribing practices that otherwise might have been prevented have proliferated. Over three years, 148 people in the analysis got prescriptions from 30 or more prescribers. The average person received medications from two. Dentists supplied most of the opioids.
Prescribers gave 4,270 people three drugs in the same month that could be dangerous if taken together. Often, patients received the drugs from different doctors, who did not coordinate care with other providers.
Patients can pay for excessive amounts of painkillers with Medicare and Medicaid. In a review of Medicare prescriptions in other states, the Office of Inspector General found four prescribers who prescribed opiods to more than 136 patients. The 2,823 prescriptions cost the program $336,000.
Prescriptions to Oregonians for amphetamines, a type of stimulant, rose by about 10% from the first half of 2017 to 2018.
Abuse of other drugs besides opioids are on the rise. In 2017, prescriptions for gabapentin, a drug used to treat seizures, within Oregon’s Medicaid program rose by 50% from the previous year. The drug can enhance the euphoric effects of opioids, but can also be deadly. More than 70% of states track gabapentin and other Schedule Vdrugs (the lowest classification of controlled substances), but Oregon does not.
Stimulants might become the next prescription drug epidemic, the audit noted. Around 16% of college students nationwide say they abuse stimulants, includingmedication for attention deficit hyperactivity disorder, which many use to achieve better grades. Most use prescriptions from friends. Prescriptions to Oregonians for amphetamines, a type of stimulant, rose by about 10% from the first half of 2017 to 2018.
Some states give doctors a report card that shows how their prescribing practices compare with those of their peers. Oregon does not. The audit recommended that the state’s monitoring program adopt this strategy.
It also recommended 11 other strategies including adding drugs, such as gabapentin, to the monitoring program, expanding data access to authorities and providing training for providers on how to access the database.
The Oregon Health Authority agreed with all of the recommendations and set deadlines to meet them, but some state laws must be changed before that can happen.
To subscribe to Oregon Business, click here.
